「コロナウイルス2019感染症はどのような機序で脳に影響を及ぼすか」
『アメリカ医師会雑誌』 2021年 3月 26日号
How COVID-19 Affects the Brain
Maura Boldrini, MD, PhD; Peter D. Canoll, MD, PhD; Robyn S. Klein, MD, PhD
JAMA Psychiatry. 2021; 78 (6): 682 - 683. doi:10.1001/jamapsychiatry.2021.0500
March 26, 2021
「アメリカ医師会雑誌」(THe Journal of American Medical Association, JAMA)の 2021年 3月 26日号に掲載された精神医学分野の論文である。広川による和訳を付して、以下に本文を示す。なお筆者(広川)の訳はこなれた日本語で分かりやすく記述することを重視したため、必ずしも逐語訳にはなっていない。文意を通じやすくするために補った語は、ブラケット [ ] で囲った。
| How COVID-19 Affects the Brain | |||
| (コロナウイルス2019感染症はどのような機序で脳に影響を及ぼすか) | |||
| COVID-19 has resulted in more than 120 million cases and 2.6 million
deaths to date. Respiratory and gastrointestinal symptoms are accompanied
by short- and long-term neuropsychiatric symptoms (NPs) and long-term brain
sequelae. |
コロナウイルス2019感染症はこれまでに1億2000万人以上に感染し、260万人の死者を出した。本疾患は呼吸器症状、消化器症状に加え、短期的・長期的精神神経症状と、長期に亙る脳の後遺症を伴う。 |
||
| Some patients present with anosmia, cognitive and attention deficits
(ie, brain fog), new-onset anxiety, depression, psychosis, seizures, and
even suicidal behavior (1, 2). These present before, during, and after respiratory symptoms and are
unrelated to respiratory insufficiency (1), suggesting independent brain damage. Follow-ups conducted in Germany
and the United Kingdom found post–COVID-19 NPs in 20% to 70% of patients,
even in young adults, and lasting months after respiratory symptoms resolved
(1), suggesting brain involvement persists. |
患者によっては無臭覚症、認知機能と注意機能の障害(ブレイン・フォグ)、初発の不安障害、抑鬱、精神病、発作を発症し、自殺行動に至る場合さえある(1, 2)。これらの症状は呼吸器症状に先行することも、同時に発症することも、遅れて発症することもあり、呼吸器系の機能不全とは関連が無い(1)ゆえに、呼吸器系とは無関係な脳の損傷を示唆している。ドイツとイギリスで実施された追跡調査によると、コロナウイルス2019感染症患者の 20パーセントないし
70パーセントに精神神経系の症状が残っている。これらの症状は成人の若年層にも現われ、呼吸器症状が収まっても数か月に亙って続く(1)ことから、脳への影響が長引くことを示している。 |
||
| Entering through angiotensin-converting enzyme 2 receptors (2), SARS-CoV-2 can damage endothelial cells leading to inflammation, thrombi,
and brain damage. Moreover, systemic inflammation leads to decreased monoamines
and trophic factors and activation of microglia, resulting in increased
glutamate and N-methyl-D-aspartate (NMDA)(3) and excitotoxicity (Figure). These insults induce new-onset or re-exacerbation of preexisting NPs. |
コロナウイルス2019(SARS-CoV-2)はアンギオテンシン変換酵素2(angiotensin-converting enzyme
2, ACE2)受容体から血管内皮細胞に侵入し(2)、内皮細胞の損傷、血栓、脳の損傷を惹き起こす。さらに全身性の炎症によってモノアミン(神経伝達物質の総称)と栄養因子の減少を招くとともに、ミクログリア(小膠細胞。中枢神経系に常在するマクロファージ)を活性化し、グルタミン酸とN-メチル-D-アスパラギン酸(N-methyl-D-aspartate,
NMDA)(3)を増加させることで、興奮毒性を惹き起こす(図参照)。これらの損傷によって新しい精神神経症状が始まり、あるいは既に存在していた精神神経症状が再び悪化する。 |
||
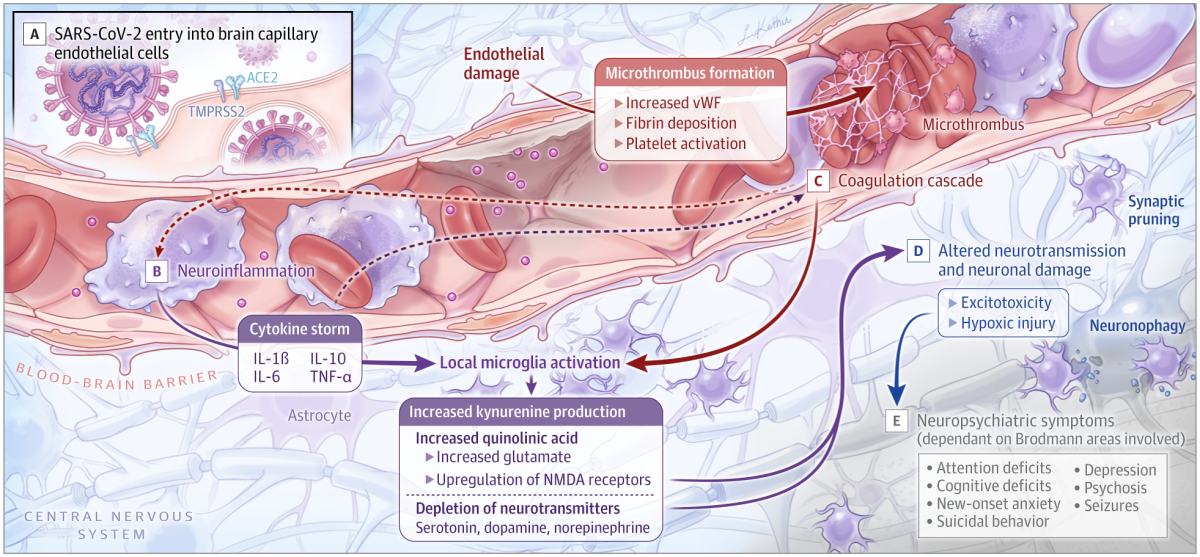
| Figure. Brain Vascular Injury, Neurotransmitter System Dysfunction, Thrombotic Events, Neuronal Damage, and Neuropsychiatric Symptoms | 図 脳血管の受傷、神経伝達系の機能不全、血栓の発生、神経損傷、精神神経系症状の発生 | ||
 |
|||
| A, SARS-CoV-2 invades endothelial cells via transmembrane angiotensin-converting enzyme 2 (ACE2) receptor, enabled by transmembrane protease, serine 2 (TMPRSS2). | A. II 型膜貫通型セリンプロテアーゼ(TMPRSS2)の働きにより、コロナウイルス2019(SARS-CoV-2)がアンギオテンシン変換酵素2(ACE2)受容体から内皮細胞に侵入する。 | ||
| B, Cytokine elevation and microglia activation result in increased kynurenine, quinolinic acid, and glutamate, and neurotransmitter depletion. | B. サイトカインが上昇し、ミクログリアが活性化することで、キヌレニン、キノリン酸、グルタミン酸が増加した結果、神経伝達物質が枯渇する。 | ||
| C, Coagulation cascade and elevation of von Willebrand factor (vWF) lead to thrombotic events. | C. 凝固カスケードとフォン・ヴィレブラント因子(vWF)の上昇が血栓発生に繋がる。 | ||
| D, Altered neurotransmission, excitotoxicity by increased glutamate, and hypoxic injury contribute to neuronal dysfunction and loss. | D. 神経伝達の変調、グルタミン酸の増加、低酸素状態による受傷のために、神経の機能不全と逸失が起こる。 | ||
| E, Neuropsychiatric symptoms differ depending on the Brodmann area involved. | E. 精神神経症状の様態は、関係するブロードマン領域により異なる。 | ||
| IL indicates interleukin; NMDA, N-methyl-D-aspartate; TNF, tumor necrosis factor. | 註 ILはインターロイキン、NMDAはN-メチル-D-アスパラギン酸、 TNFは腫瘍壊死因子を指す。 | ||
| Does the Virus Invade the Brain? | コロナウイルス2019は脳に侵入するか | ||
| SARS-CoV-2 is known to penetrate the olfactory mucosa, causing loss
of smell, and may enter the brain, migrating from the cribriform plate
along the olfactory tract (2) or through vagal or trigeminal pathways; however, definitive evidence
for this is lacking. SARS-CoV-2 could pass the blood-brain barrier (BBB)
because inflammatory cytokines induce BBB instability or via monocytes
(4). It could reach brain tissue via circumventricular organs (CVOs),
midline structures around the third and fourth ventricles, that monitor
blood and cerebral spinal fluid content via fenestrated capillaries lacking
the junctional proteins expressed in the BBB. |
コロナウイルス2019は嗅粘膜に侵入して嗅覚消失を起こすことが知られているが、篩板から嗅索を通り(2)、あるいは迷走神経または三叉神経を通って、脳に侵入する可能性がある。ただしこのことに関して決定的な証拠は見つかっていない。コロナウイルス2019は血液脳関門(the
blood-brain barrier, BBB)を通過できるが、これは炎症性サイトカインによって血液脳関門が不安定になることによって、あるいは単球を経由することによって(4)可能になる。ウイルスは脳室周囲器官(circumventricular organs, CVOs)を経由して脳組織に到達し得る。脳室周囲器官は第三・第四脳室付近の正中線上にある構造で、有窓性毛細血管を通して血液と脳脊髄液の内容を監視しているが、血液脳関門に発現する細胞結合蛋白質を欠いている。 |
||
| Viral RNA was detected by reverse transcription–quantitative real-time
polymerase chain reaction but not by in situ hybridization in medulla and
cerebellum (2), located next to the area postrema, a CVO that controls emetic responses
to toxins. SARS-CoV-2 protein has been found in brain vascular endothelium
but not in neurons or glia (2). Thus, detected viral RNA may represent contamination by vasculature
in leptomeninges and Virchow-Robin spaces. |
最後野(area postrema 菱形窩の後端。血液脳関門が無い)は脳室周囲器官のひとつで、有毒物質に対する嘔吐反応を制御する。延髄と小脳は最後野に隣接している。本研究においてウイルスRNAが検出されたのはRT-PCRを用いた定量的分析によるもので、延髄や小脳における
in situハイブリダイゼーションにはよらない (2)。コロナウイルス2019の蛋白質は脳血管の内皮細胞で検出されたが、ニューロン及びグリア細胞には見つからなかった。したがって検出されたRNAは、脳脊髄膜及びVirchow-Robin
腔(血管周囲腔)の血管系による汚染の可能性がある。 |
||
| Histopathologic analysis of whole human brain showed microglial nodules and phagocytosis of neurons (neuronophagia) in brain stem and less frequently in cortex and limbic structures, associated with sparse lymphocytic infiltration, and no correlations between histopathologic findings and levels of viral messenger RNA in the same brain (5). While ageusia, nausea, and vomiting may be related to CVO and brain stem viral invasion, other short-term and long-lasting NPs are more likely due to neuroinflammation and hypoxic injury. Brain stem involvement may explain persistent autonomic abnormalities and anxiety. | ヒトの脳全体に組織病理学的分析をおこなったところ、主に脳幹で、時に皮質と辺縁系で、ミクログリアの結節とニューロンの貪食が見つかった。これらの結節と貪食は散発性のリンパ球浸潤と関連を有し、同じ脳で見つかった組織病理学的徴候及びウイルスのmRNAとは相関を持たない(5)。味覚消失、悪心、嘔吐は脳室周囲器官や脳幹と関連する可能性がある一方、短期的及び長期的な他の精神神経症状は神経炎症及び低酸素症によって起きた障害のためである可能性が高い。自律神経失調症や不安症が続く場合は、脳幹の関与で説明できる可能性がある。 | ||
| Cytokines and Microglia Activation Lead to Neurotoxicity | サイトカインとミクログリア活性化による神経毒性 | ||
| Patients with severe COVID-19 infection have been reported to experience
a severe cytokine storm, with increased serum levels of proinflammatory
cytokines including interleukin (IL) 1, IL-6, IL-10, and tumor necrosis
factor (TNF)-α. TNF-α can directly cross the BBB by transport (increased
BBB permeability due to cytokine-induced damage)(4) or CVOs. Once across the BBB, cytokines activate microglia and astrocytes (6). In addition to phagocytosing damaged cells, activated microglia
secrete inflammatory mediators, including glutamate, quinolinic acid, ILs,
complement proteins, and TNF-α (7). Increased quinolinic acid results in higher glutamate and upregulation
of NMDA receptors, possibly inducing altered learning, memory, neuroplasticity,
hallucinations, and nightmares. Excitotoxicity and neuronal loss result
in region- and neurotransmitter-specific NPs. |
これまでの報告によると、コロナウイルス2019感染症の重症患者は重篤なサイトカインストームを起こし、IL(インターロイキン)-1、IL-6、IL-10、TNF(腫瘍壊死因子)-αを初めとする炎症誘発性サイトカインの血清中レベルが高まる。血液脳関門がサイトカインで損傷すると浸透性が高まるために(4)、TNF-αは膜輸送によって血液脳関門を直接的に通過できるし、脳室周囲器官を経由する場合もある。血液脳関門をいったん通過すると、サイトカインはミクログリアと星状細胞を活性化する(6)。活性化したミクログリアは損傷した細胞を貪食するだけでなく、グルタミン酸、キノリン酸、インターロイキン、補体、TNF-αを初めとする炎症性メディエーターを分泌する(7)。キノリン酸が増加すると、グルタミン酸濃度が上昇するとともに、NMDA受容体の応答能が向上し、学習能力や記憶力や神経可塑性に変調をきたしたり、幻覚や悪夢が生じたりする可能性がある。興奮毒性と神経の消失により、脳の領域と神経伝達物質の種類に応じた神経精神症状が生じる。 |
||
| Inflammation and NPs | 炎症と神経精神症状 | ||
| Increased inflammation activates the enzyme indoleamine dioxygenase,
which metabolizes tryptophan to kynurenine rather than serotonin (3). Reduced neurotransmitter release was demonstrated in patients treated
with interferon alfa who exhibited increased positron emission tomography
fluorodopa 18F uptake and decreased turnover in caudate and putamen, which correlated
with depression and fatigue severity. Similarly, interferon- or IL-based
immunotherapy can induce depression. Inflammation leads to blunted monoamine
neurotransmission, anhedonia, negative cognitive, psychomotor and neurovegetative
symptoms, depression, and suicidal behavior, which poorly respond to conventional
antidepressants (3). |
炎症の悪化により、インドールアミン-ジオキシゲナーゼが活性化する。インドールアミン-ジオキシゲナーゼはトリプトファンをセロトニンではなくキヌレニンに代謝する酵素である(3)。インターフェロン・アルファによる治療を受けた患者は、神経伝達物質の放出量が減ることが示された。フルオロドーパ(18F)を使用した陽電子放出断層撮影(positron emission tomography, PET)において、インターフェロン・アルファによる治療を受けた患者は、フルオロドーパの取り込みが増え、尾状核と被核における代謝が減ることが示された。この徴候は抑鬱と疲労の大きさに相関していた。これと同様に、インターフェロンに基づく免疫療法あるいはインターロイキンに基づく免疫療法を受けた患者は抑鬱状態になり得る。炎症が起こるとモノアミンによる神経伝達が鈍り、快感消失、負の認知性・精神運動性・自立神経性症状、抑鬱、自殺的行動につながるが、これらは従来の抗鬱剤を投与しても容易に改善しない(3)。 |
||
| In individuals who attempt suicide and have major depressive disorder,
studies found elevated plasma kynurenine, high IL-1 and IL-6 levels in
blood, cerebral spinal fluid, and brain, and increased serum C-reactive
protein correlating with brain glutamate levels. TNF-α and IL-6 levels
may predict negative and depressive symptoms in people at risk of psychosis,
and higher IL-6 correlates with smaller hippocampus volume. Elevated IL-1β
signaling decreases hippocampal neurogenesis and increases apoptosis in
mammals. Suicide decedents with major depressive disorder have increased
proinflammatory and decreased neurogenesis markers in postmortem hippocampus
(8), together with smaller dentate gyrus, fewer granule neurons, and
neural progenitor cells (9). Therefore, neuroinflammation may contribute to the pathogenesis
of NPs reducing neurotransmitters and neurotrophins and increasing excitotoxicity
(3). |
研究結果が示すところによると、自殺を試み、大鬱病性障害を有する人は、血漿中のキヌレニンが上昇し、血中。脳脊髄液中、脳中の IL-1と IL-6濃度が大きくなり、脳中のグルタミン酸濃度に相関して血清中のC反応性蛋白も増加する。精神病のリスクがある人の場合、TNF-α と IL-6 の濃度を測れば抑鬱的で好ましくない症状を予測できる可能性がある。IL-6の増加と海馬の体積減少は相関する。哺乳動物において、IL-1βからのシグナルが増えると海馬における神経形成が減少し、アポトーシスが増加する。大鬱病性障害を患って自殺した人を剖検すると、海馬に炎症誘発性マーカーが増え、神経形成マーカーが減少している(8)。また歯状回は縮小し、顆粒神経細胞と神経前駆細胞は減少している(9)。それゆえ神経が炎症を起こせば、神経伝達物質と神経栄養因子が減少し、また興奮毒性が強まって、神経精神症状の病因となる可能性がある(3)。 | ||
| Interplay of Inflammation and Coagulation | 炎症と凝血の相互作用 | ||
| Virus entrance into endothelial cells of brain vasculature activates neutrophils,
macrophages, thrombin production, and complement pathways, promoting microthrombi
deposition (2). COVID-19 brain damage shows macro– and micro–hypoxic/ischemic injury
and infarcts at autopsy (5). Moreover, the complement cascade mediates synaptic pruning by microglia
following viral infections (7). Therefore, NPs of COVID-19 could result from microstrokes and neuronal
damage, and symptoms consequently differ depending on the brain region
involved. Mechanisms of COVID-19 brain damage may resemble those involved
in traumatic brain injury, where a combination of proinflammatory status
and microvascular injury resulting in neuronal loss have been implicated
in the pathogenesis of suicidal behavior (10). Conversely, a successful clinical outcome would result from an
initial immune response involving toll receptors and blunted nonpriming
or low-priming delayed inflammation. |
脳血管系の内皮細胞にウイルスが侵入すると、好中球とマクロファージが活性化され、トロンビンの産生が促進される。また補体活性化シグナルの伝達経路が活性化し、微小血栓の排除を促進する(2)。コロナウイルス2019感染症による脳損傷には、様々な規模の低酸素状態あるいは虚血による受傷と梗塞が見られる(5)。さらにウイルス感染に引き続き、補体カスケードが媒介となって、ミクログリアによるシナプス剪定がおこなわれる(7)。それゆえコロナウイルス2019感染症の神経精神症状は微小な卒中と神経損傷の結果であり、それゆえ関係する脳の部位によって症状が異なる。コロナウイルス2019感染症によって脳が損傷する仕組みは、外傷性脳損傷の場合と一定の類似性を有する。外傷性脳損傷の場合、炎症が促進され、かつ微小血管の受傷によって神経消失が起こることが、自殺的行動の病因と示唆されているからだ(10)。逆に言えばトル様受容体(TLR)[が有効に発動し、]炎症が急性でなくゆっくりと進行し、次の反応を惹き起こす作用が無いかまたは小さい場合、最初の免疫応答がそのようであれば、臨床上の転帰も良好なものとなろう。 |
||
| Understanding cellular and molecular aspects of COVID-19 brain damage
could direct interventions to reduce long-term NPs. Interventions may involve
antagonists of cytokines (etanercept, infliximab), NMDA receptor (ketamine),
TNF-α and anti-inflammatory pathways (aspirin, celecoxib), and kynurenine
pathway modulators (minocycline)(3). Mitigating long-term post–COVID-19 cognitive, emotional, and behavioral
sequelae would decrease disease burden. COVID-19 neuropathology may serve
as a model for deciphering neurodegenerative processes related to neuroinflammation
in other brain diseases and developing new treatment strategies. |
コロナウイルス2019感染症による脳損傷を細胞と分子の側面から理解できれば、長期的神経精神症状を減らす治療に役立つであろう。サイトカイン阻害薬(エタネルセプト、インフリキシマブ)、NMDA受容体阻害薬(ケタミン)、TNF-α 及び炎症経路阻害薬(アスピリン、セレコキシブ)、キヌレニン経路調節因子(ミノサイクリン)が治療に使えるであろう(3)。コロナウイルス2019感染症が治癒した後、長期に亙る認知、感情、ふるまいの後遺症を軽減できれば、病気による負担を減らすことができよう。コロナウイルス2019感染症の神経病理学は他の脳疾患の神経炎症に関わる神経変性疾患の過程を解明するためのモデルとして、また新しい治療戦略を立てるためのモデルとして役立つと思われる。 |
||
Article Information
Corresponding Author: Maura Boldrini, MD, PhD, Department of Psychiatry, New York State Psychiatric Institute, Columbia University Irving Medical Center, 1051 Riverside Dr, Unit 42, New York, NY 10032 (mb928@cumc.columbia.edu).
Published Online: March 26, 2021. doi:10.1001/jamapsychiatry.2021.0500
Conflict of Interest Disclosures: Dr Boldrini is supported by the National Institutes of Health, the American Foundation for Suicide Prevention, Dr Brigitt Rok Foundation, and the Morris Stroud III Center for Study of Quality of Life in Health and Aging at Columbia University. Drs Canoll and Klein are supported by the National Institutes of Health.
Additional Contributions: We thank Helen Blair Simpson, MD, PhD (New York State Psychiatric Institute and Columbia University), for reviewing a draft of this work. Dr Simpson was not compensated.References
1.Woo MS, Malsy J, Pöttgen J, et al. Frequent neurocognitive deficits after recovery from mild COVID-19. Brain Commun. 2020;2(2):fcaa205. doi:10.1093/braincomms/fcaa205 Google Scholar
アカデミア神戸 医療関係資料 インデックスに戻る
アカデミア神戸 大人のための教養講座 インデックスに移動する
アカデミア神戸 トップページに移動する
Ἀναστασία ἡ Οὐτοπία τῶν αἰλούρων ANASTASIA KOBENSIS, ANTIQUARUM RERUM LOCUS NON INVENIENDUS